What Are Four Common Causes of Knee Pain?
Knee pain affects approximately 25% of adults over age 45 in the United States, making it one of the most prevalent musculoskeletal complaints [1]. Whether you’re experiencing occasional discomfort or chronic pain that limits your daily activities, understanding the root cause is the first step toward effective relief.
At Joint Relief Institute, we’ve treated over 40,000 patients and completed more than 400,000 procedures, giving us deep insight into what causes knee pain and how to treat it effectively without surgery.
What Is Knee Pain?
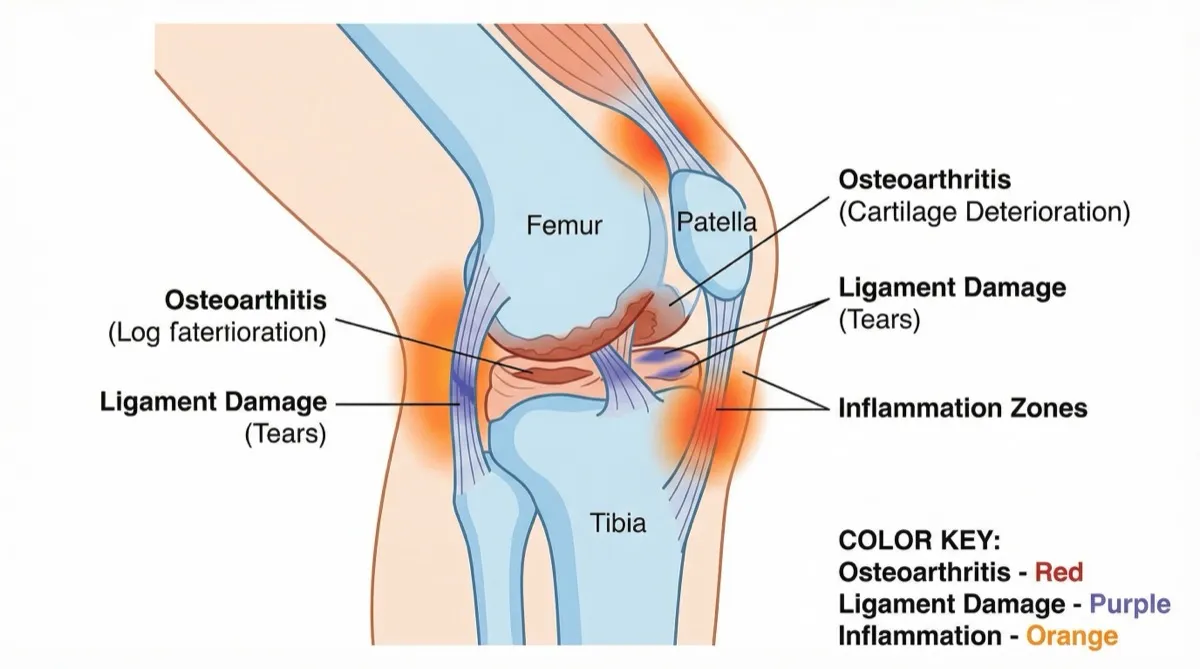
Knee pain is discomfort originating from the knee joint and surrounding structures including bones, cartilage, ligaments, tendons, and bursae. The prevalence of knee pain in global populations ranges from 10% to 60%, with rates increasing significantly with age [1]. Among adults 65 and older, nearly 37% report experiencing knee pain [2].
The knee is the largest joint in your body and bears significant stress during everyday activities. When any component of this complex joint becomes damaged or inflamed, pain can range from mild irritation to debilitating discomfort that interferes with walking, climbing stairs, or even standing.
The Four Most Common Causes of Knee Pain
1. Osteoarthritis: The Leading Cause of Chronic Knee Pain
Osteoarthritis is the most common cause of knee pain, affecting over 32.5 million Americans [3]. This degenerative joint disease occurs when the protective cartilage cushioning the ends of bones gradually wears down over time.
Prevalence and Impact:
According to research published in the Journal of Rheumatology, the pooled global prevalence of knee osteoarthritis is 22.9% in individuals aged 40 and over [4]. In the United States, an estimated 13.7 million people have symptomatic knee osteoarthritis, representing 6.9% of the population aged 25 and older [5].
The statistics become more striking when examining specific age groups. Among US adults age 60 and older, radiographic knee osteoarthritis was found in 37.4% of individuals [6]. What’s particularly concerning is that knee osteoarthritis prevalence has doubled since the mid-20th century, even when accounting for increases in longevity and body mass index [7].
Who’s at Risk:
Women experience significantly higher rates of knee osteoarthritis than men. Research shows the female-to-male ratio for prevalence is 1.69, meaning women are nearly 70% more likely to develop the condition [4]. Radiographic knee osteoarthritis was detected in 42.1% of women compared to 31.2% of men [6].
Additional risk factors include:
- Age over 50
- Obesity (increases risk up to four times) [1]
- Previous knee injuries
- Repetitive stress on the knee joint
- Genetic predisposition
- Muscle weakness around the knee
Symptoms:
People with knee osteoarthritis typically experience:
- Pain that worsens with activity and improves with rest
- Morning stiffness lasting less than 30 minutes
- Grinding or clicking sensations (crepitus)
- Swelling after prolonged activity
- Decreased range of motion
- Knee buckling or feeling unstable
Treatment Options:
At Joint Relief Institute, we specialize in viscosupplementation—hyaluronic acid gel injections that help lubricate the joint and reduce pain [8]. Unlike cortisone shots that simply mask pain, viscosupplementation treatments work by replacing lost joint fluid, providing cushioning and potentially slowing cartilage deterioration.
Research indicates that viscosupplementation demonstrates moderate but significant efficacy versus placebo, with 60-70% of patients experiencing meaningful pain relief that can last up to six months [9]. Our fluoroscopy-guided injection technique ensures precise placement of the gel directly into the joint space for optimal results.
Other effective treatments include:
- Physical therapy to strengthen supporting muscles
- Weight management to reduce joint stress
- Low-impact exercises (swimming, cycling)
- Anti-inflammatory medications
- Bracing or orthotics
2. Ligament Injuries: ACL and MCL Tears
The knee contains four major ligaments that provide stability: the anterior cruciate ligament (ACL), posterior cruciate ligament (PCL), medial collateral ligament (MCL), and lateral collateral ligament (LCL). Injuries to these structures, particularly the ACL, are extremely common.
Prevalence:
The ACL is the most commonly injured ligament in the knee, accounting for nearly half of all knee injuries [10]. The annual incidence in the United States is approximately 1 in 3,500 people, with approximately 400,000 ACL reconstructions performed yearly [10]. In female athletes, the injury rate is 4.5 times higher than in males [10].
Common Causes:
Ligament injuries typically occur during:
- Sudden changes in direction while running (cutting movements)
- Abrupt stopping or slowing down
- Landing incorrectly from a jump
- Direct impact to the knee during contact sports
- Pivoting with a planted foot
Sports with the highest ACL injury rates include soccer, football, basketball, skiing, and gymnastics. These activities involve frequent cutting, pivoting, and jumping movements that stress the ligaments beyond their normal capacity.
Symptoms:
When a ligament tears, people often report:
- A loud “pop” at the time of injury
- Immediate, severe pain
- Rapid swelling within hours
- Inability to bear weight on the affected leg
- Feeling of knee instability or “giving way”
- Loss of full range of motion
Associated Complications:
About half of all ACL injuries occur along with damage to other structures, particularly the meniscus or articular cartilage [11]. Research shows that at 10 to 20 years after ACL or meniscus tear diagnosis, approximately 50% of patients develop osteoarthritis with associated pain and functional impairment [12].
Treatment Approaches:
Treatment depends on injury severity, patient age, and activity level:
Conservative (Non-surgical):
- Physical therapy focusing on strengthening and stability
- Bracing to provide external support
- Activity modification
- Anti-inflammatory medications
Surgical:
- ACL reconstruction using grafts
- Minimally invasive arthroscopic techniques
- Post-operative rehabilitation (typically 6-9 months)
For patients who develop post-traumatic osteoarthritis following ligament injuries, Joint Relief Institute offers viscosupplementation therapy as a non-surgical option to manage pain and improve function.
3. Meniscus Tears: Cartilage Damage
The meniscus consists of two C-shaped pieces of cartilage that act as shock absorbers between your thighbone and shinbone. Meniscus tears are among the most common knee injuries, particularly in athletes and older adults.
Prevalence:
Knee meniscal injuries have an incidence of 61 cases per 100,000 people, with risk factors including male sex and age over 40 [13]. Medial meniscal tears are more common than lateral tears [13]. Meniscus tears are frequently found in patients with ACL ruptures, often occurring as combined injuries [14].
How Tears Occur:
Meniscus tears develop through two primary mechanisms:
Acute Tears (Traumatic):
- Forceful twisting or rotating of the knee
- Sudden pivoting movements during sports
- Deep squatting or kneeling
- Direct trauma from tackles or falls
Degenerative Tears:
- Age-related weakening of cartilage tissue
- Gradual deterioration from years of use
- Often occurring during routine activities in people over 40
The mechanism typically involves a combination of axial loading (weight-bearing) and rotational forces that create shearing stress on the meniscus [13].
Symptoms:
Meniscus tear symptoms include:
- Pain along the joint line
- Swelling that develops over 24-48 hours
- Popping or clicking sensations
- Knee locking or catching
- Inability to fully straighten the knee
- Pain when twisting or rotating the knee
Treatment Options:
Conservative Management:
- Rest, ice, compression, elevation (RICE protocol)
- Physical therapy to strengthen quadriceps and hamstrings
- Anti-inflammatory medications
- Activity modification
Surgical Intervention:
- Arthroscopic meniscus repair (preserving tissue)
- Partial meniscectomy (removing damaged portion)
- Typically outpatient procedures with faster recovery
Long-term Considerations:
Meniscus tears significantly increase osteoarthritis risk. Even after surgical treatment, many patients develop degenerative changes over time. This is where Joint Relief Institute’s viscosupplementation treatments become particularly valuable—providing a non-surgical option for managing pain that develops years after the initial injury.
4. Patellofemoral Pain Syndrome: Runner’s Knee
Patellofemoral pain syndrome (PFPS), commonly called “runner’s knee,” refers to pain behind or around the kneecap. It’s one of the most common causes of anterior knee pain, particularly in active individuals and athletes.
Prevalence:
The estimated annual prevalence of PFPS is 22.7% in the general population and 28.9% in adolescents [15]. In the United States, incidence ranges from 3% to 6%, representing approximately 1.75 million patients annually, with females accounting for 55% of cases [15].
Causes and Risk Factors:
The etiology of patellofemoral syndrome is multifactorial. Contributing factors include:
Biomechanical Issues:
- Quadriceps weakness
- Hip abductor and external rotator dysfunction
- Tightness of the iliopsoas, hamstrings, or iliotibial band
- Foot hyperpronation (excessive inward rolling)
- Patellar malalignment or hypermobility
- Leg length discrepancy [15]
Activity-Related Factors:
- Sudden increases in training intensity or volume
- Running on hard or uneven surfaces
- Poor footwear without adequate support
- Repetitive jumping or squatting movements
Symptoms:
Patients with PFPS typically complain of:
- Generalized anterior knee pain
- Pain aggravated by loading a flexed knee (running, stairs, squatting)
- Discomfort during prolonged sitting with knees bent (“theater sign”)
- Grinding or crunching sensations behind the kneecap
- Pain that improves with rest
Treatment and Prognosis:
The majority of patients with PFPS experience resolution of symptoms with conservative treatments [15]:
Physical Therapy:
- Quadriceps strengthening exercises
- Hip stabilization training
- Hamstring and IT band stretching
- Patellar taping or bracing
Activity Modification:
- Gradual return to activity
- Cross-training with low-impact exercises
- Proper footwear selection
- Running form analysis and correction
Additional Interventions:
- NSAIDs for pain and inflammation
- Ice after activity
- Orthotics for foot alignment issues
While PFPS rarely requires surgical intervention, some cases can be resistant to therapy and persist for years. For patients with chronic symptoms, addressing any underlying biomechanical issues is essential for long-term relief.
Other Causes of Knee Pain
While osteoarthritis, ligament injuries, meniscus tears, and patellofemoral pain syndrome represent the four most common causes, several other conditions can produce knee discomfort:
Bursitis: Inflammation of the small fluid-filled sacs (bursae) that cushion the knee joint. Prepatellar bursitis has an annual incidence of at least 10 per 100,000 people, primarily affecting men aged 40-60 who kneel frequently for work [16].
Tendinitis: Inflammation of the tendons around the knee, particularly the patellar tendon (jumper’s knee) or quadriceps tendon, typically caused by overuse and repetitive stress.
IT Band Syndrome: Irritation of the iliotibial band where it crosses the outside of the knee, common in runners and cyclists.
Gout or Pseudogout: Crystal deposits in the joint causing sudden, severe pain and swelling.
Baker’s Cyst: Fluid-filled swelling behind the knee that can cause tightness and discomfort.
Fractures: Breaks in the kneecap, femur, or tibia from trauma or stress injuries.
When to Seek Medical Attention
While minor knee pain often resolves with rest and home care, certain symptoms warrant professional evaluation:
Seek immediate medical attention if you experience:
- Severe pain that prevents weight-bearing
- Obvious deformity of the knee joint
- Inability to fully extend or flex the knee
- Significant swelling within hours of injury
- Signs of infection (fever, redness, warmth)
- Knee giving way or buckling during normal activities
Schedule an appointment with a specialist if:
- Knee pain persists beyond a few weeks
- Pain interferes with daily activities or sleep
- Over-the-counter pain medications provide insufficient relief
- Swelling recurs repeatedly
- You notice progressive worsening of symptoms
How Joint Relief Institute Can Help
At Joint Relief Institute, we specialize in non-surgical treatment for knee pain caused by osteoarthritis and degenerative joint conditions. Our core treatment—viscosupplementation with hyaluronic acid gel injections—provides an effective alternative to surgery for many patients.
What Sets Us Apart:
Fluoroscopy-Guided Precision: Unlike injections performed “blind” based on anatomical landmarks, we use real-time X-ray guidance to ensure the gel is placed precisely where it’s needed for optimal results.
Experienced Specialists: With over 400,000 procedures completed, our physicians have refined techniques that maximize comfort and effectiveness.
Comprehensive Approach: We develop individualized treatment plans that may include multiple injections over a series of weeks, combined with physical therapy recommendations and lifestyle modifications.
Proven Results: Our 4.9 Google rating reflects the thousands of patients who’ve experienced significant pain relief and improved mobility through our treatments.
Insurance Acceptance: We accept Medicare and most major insurance plans, making treatment accessible to those who need it.
Who Benefits from Our Treatment:
Viscosupplementation is particularly effective for patients with:
- Mild to moderate knee osteoarthritis
- Pain not adequately controlled by medications or physical therapy alone
- Desire to avoid or delay surgical intervention
- Previous knee injuries leading to post-traumatic arthritis
- Active lifestyles limited by knee discomfort
Take the First Step Toward Relief
If knee pain is limiting your activities and quality of life, you don’t have to accept it as an inevitable part of aging. With advancements in non-surgical treatments like viscosupplementation, many patients experience significant improvement without the risks, costs, and recovery time associated with surgery.
Contact Joint Relief Institute today at (800) 238-9307 to schedule a consultation. Our specialists will conduct a thorough evaluation, explain your treatment options, and develop a personalized plan to help you get back to the activities you love.
Don’t let knee pain hold you back any longer. Call us today and discover why over 40,000 patients have trusted Joint Relief Institute for effective, non-surgical joint pain relief.
Sources
-
Knee Pain Centers of America. “Knee Pain Prevalence Statistics.” 2025. https://www.kneepaincentersofamerica.com/blog/knee-pain-prevalence-statistics
-
Knee Pain Centers of America. “Statistics on Knee Pain by Age Group.” 2025. https://www.kneepaincentersofamerica.com/blog/statistics-on-knee-pain-by-age-group
-
Osteoarthritis Action Alliance, University of North Carolina. “OA Prevalence and Burden.” 2024. https://oaaction.unc.edu/oa-module/oa-prevalence-and-burden/
-
Cui A, et al. “Global, regional prevalence, incidence and risk factors of knee osteoarthritis in population-based studies.” PMC, 2020. https://pmc.ncbi.nlm.nih.gov/articles/PMC7704420/
-
Dillon CF, et al. “Prevalence of knee osteoarthritis in the United States: arthritis data from the Third National Health and Nutrition Examination Survey 1991-94.” The Journal of Rheumatology, 2006. https://pubmed.ncbi.nlm.nih.gov/17013996/
-
Zhang Y, Jordan JM. “Epidemiology of Osteoarthritis.” PMC, 2010. https://pmc.ncbi.nlm.nih.gov/articles/PMC2920533/
-
Wallace IJ, et al. “Knee osteoarthritis has doubled in prevalence since the mid-20th century.” PNAS, 2017. https://www.pnas.org/doi/10.1073/pnas.1703856114
-
Hospital for Special Surgery. “What to Know About Knee Gel Injections (Viscosupplementation).” 2025. https://www.hss.edu/health-library/conditions-and-treatments/knee-gel-injections-viscosupplementation
-
Colen S, et al. “A Comprehensive Review of Viscosupplementation in Osteoarthritis of the Knee.” PMC, 2021. https://pmc.ncbi.nlm.nih.gov/articles/PMC8567800/
-
Evans J, Nielson JL. “Anterior Cruciate Ligament Knee Injury.” StatPearls, NCBI Bookshelf, 2024. https://www.ncbi.nlm.nih.gov/books/NBK499848/
-
American Academy of Orthopaedic Surgeons. “Common Knee Injuries.” OrthoInfo, 2024. https://orthoinfo.aaos.org/en/diseases—conditions/common-knee-injuries/
-
Lohmander LS, et al. “The long-term consequence of anterior cruciate ligament and meniscus injuries: osteoarthritis.” PubMed, 2007. https://pubmed.ncbi.nlm.nih.gov/17761605/
-
PM&R KnowledgeNow. “Meniscus Injuries of the Knee.” American Academy of Physical Medicine and Rehabilitation, 2024. https://now.aapmr.org/meniscus-injuries-of-the-knee/
-
Kang J, et al. “Association of Meniscus Injuries in Patients With Anterior Cruciate Ligament Injuries.” PMC, 2022. https://pmc.ncbi.nlm.nih.gov/articles/PMC9275808/
-
Waryasz GR, McDermott AY. “Patellofemoral pain syndrome (PFPS): a systematic review of anatomy and potential risk factors.” PMC, 2018. https://pmc.ncbi.nlm.nih.gov/articles/PMC5764329/
-
Williams CH, Sternard BT. “Bursitis.” StatPearls, NCBI Bookshelf, 2024. https://www.ncbi.nlm.nih.gov/books/NBK513340/


