Osteoarthritis Knee Treatment: Every Option From Conservative Care to Surgery
Nearly 530 million people worldwide live with osteoarthritis, and the knee is the most commonly affected joint [1]. If you’ve been diagnosed with knee osteoarthritis — or suspect you have it — you’re facing a flood of treatment advice, much of it conflicting. Some doctors tell you to “just take ibuprofen.” Others push you straight toward knee replacement.
The reality is more nuanced. Osteoarthritis knee treatment in 2026 spans a wide spectrum, from daily exercise habits to advanced injection therapies to surgical intervention. The right approach depends on your stage of disease, your activity goals, and how your body responds to each treatment step. After performing over 400,000 procedures and treating more than 40,000 patients since 2015, I’ve seen what works, what doesn’t, and what the research consistently supports.
This guide walks through every major treatment option — ranked from the most conservative to the most interventional — so you can make an informed decision with your physician.
What Is Knee Osteoarthritis?
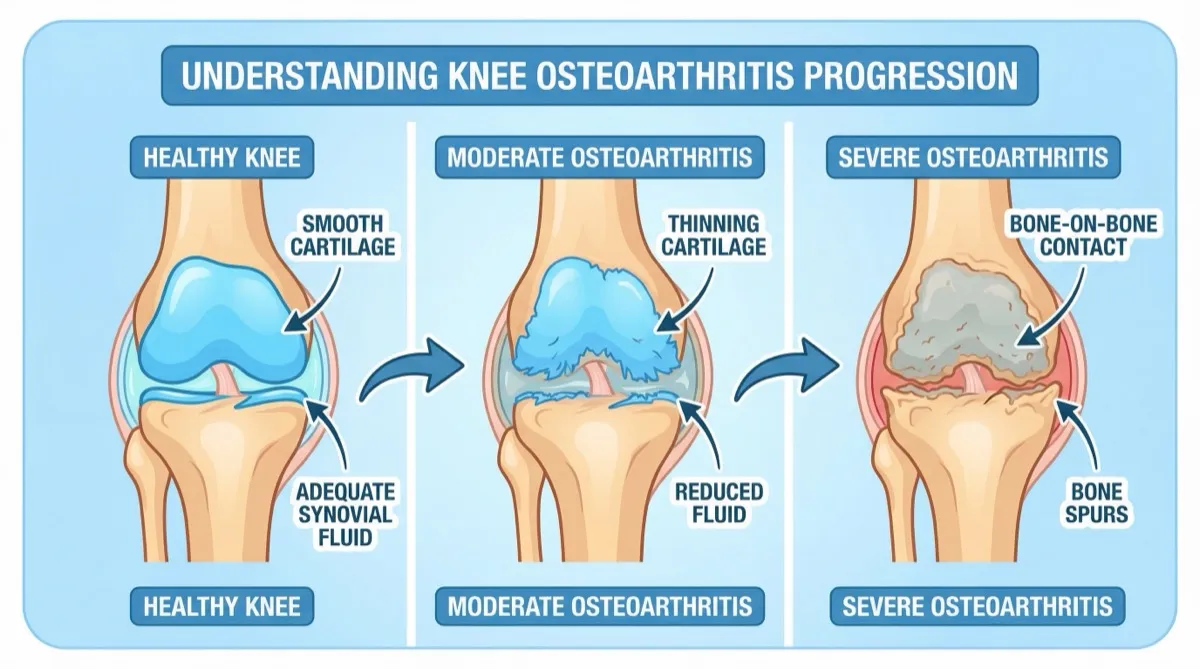
Osteoarthritis (OA) is a degenerative joint disease in which the cartilage that cushions the ends of your bones gradually breaks down. In the knee, this means the smooth, slippery surface that allows your femur (thighbone) and tibia (shinbone) to glide against each other becomes rough, thin, and eventually worn away [1].
As cartilage deteriorates, your body responds with inflammation. Bone spurs (osteophytes) form along joint margins. The synovial fluid that lubricates your knee loses its viscosity and volume. The result is pain, stiffness, swelling, and reduced range of motion that worsens over months and years.
Who Gets Knee Osteoarthritis?
Knee OA is not just an “aging” disease, though age is the strongest risk factor. The lifetime risk of developing symptomatic knee osteoarthritis is approximately 45% — affecting 40% of men and 47% of women [1]. Key risk factors include:
- Age: Prevalence rises sharply after 50, affecting 33.6% of adults 65 and older [1]
- Weight: Every pound of excess body weight adds 3 to 6 pounds of force across the knee joint [2]
- Previous injury: A torn meniscus, ACL tear, or fracture involving the knee significantly increases OA risk
- Gender: Women are more likely to develop knee OA, particularly after menopause
- Genetics: Family history accounts for an estimated 40-65% of OA risk
- Occupation: Jobs involving prolonged kneeling, squatting, or heavy lifting accelerate cartilage wear
Symptoms That Signal Knee Osteoarthritis
The hallmark symptoms develop gradually and typically include. If these symptoms have persisted for three months or more, see our guide on chronic knee pain treatment for a full breakdown of treatment options:
- Morning stiffness lasting less than 30 minutes (unlike rheumatoid arthritis, which lasts longer)
- Pain with activity that improves with rest in early stages
- Crepitus — a grinding or crunching sensation when bending the knee
- Swelling around the joint, particularly after extended use
- Decreased range of motion — difficulty fully bending or straightening the knee
- Instability or a feeling that the knee might “give way”
If these symptoms sound familiar, your doctor can confirm the diagnosis with a physical exam and X-rays.
How Osteoarthritis Progresses: The 4 Stages
Not all knee arthritis is the same. Physicians use the Kellgren-Lawrence (KL) grading system to classify severity based on X-ray findings [3]. Understanding your stage is essential because it determines which osteoarthritis treatment options are most appropriate.
Stage 1: Doubtful (KL Grade 1)
- Minor bone spur formation
- No significant joint space narrowing
- You may feel occasional stiffness after prolonged sitting
- Treatment focus: Lifestyle modification, exercise, weight management
Stage 2: Mild (KL Grade 2)
- Definite bone spurs visible on X-ray
- Possible early joint space narrowing
- Pain after long walks, climbing stairs, or kneeling
- Treatment focus: Exercise, physical therapy, NSAIDs as needed, bracing
Stage 3: Moderate (KL Grade 3)
- Multiple bone spurs
- Definite joint space narrowing
- Some subchondral sclerosis (bone hardening beneath cartilage)
- Frequent pain, stiffness, and swelling that interfere with daily activities
- Treatment focus: Viscosupplementation, physical therapy, activity modification, cortisone for flare-ups
Stage 4: Severe (KL Grade 4)
- Large bone spurs
- Marked joint space narrowing or complete loss
- Significant bone-on-bone contact
- Pain at rest, severe functional limitation
- Treatment focus: Viscosupplementation (multiple courses), combination therapy, surgical evaluation when conservative measures fail
An important point: many patients told they are “bone-on-bone” actually have KL Grade 3 disease — where meaningful cartilage remains and non-surgical treatment can still provide substantial relief. For a deeper dive, see our guide on gel injections for bone-on-bone knees.
Non-Surgical Osteoarthritis Knee Treatment Options
The following treatments are listed from most conservative to most interventional. Evidence-based guidelines consistently recommend starting with foundational therapies and escalating as needed [1][2].
1. Exercise and Physical Therapy
The evidence: Exercise is the single most supported non-surgical intervention for knee osteoarthritis. A comprehensive review of over 200 studies found that aerobic exercise — walking, cycling, swimming — offers the best combination of pain relief and mobility improvement [4]. Resistance training and aquatic therapy also show strong evidence. Supervised physical therapy delayed total knee replacement in 95% of patients who received it [5].
What works best:
- Low-impact aerobic exercise: Walking 30 minutes most days, cycling, swimming, or elliptical training
- Quadriceps strengthening: The muscles at the front of your thigh are the primary stabilizers of your knee. Strengthening them reduces load on the joint
- Flexibility training: Gentle stretching and range-of-motion exercises to combat stiffness
- Balance work and Tai Chi: Moderate evidence supports improved stability and reduced fall risk [2]
- Aquatic therapy: Exercising in water reduces joint stress by up to 50% while providing resistance for strengthening
The catch: Exercise requires consistency. Benefits diminish when you stop. But it costs nothing, has no side effects, and should be part of every osteoarthritis treatment plan regardless of disease stage.
2. Weight Management
The evidence: Excess weight is both a cause and an accelerator of knee OA. Weight reduction is “strongly recommended as a core intervention” by virtually every clinical guideline [2]. Losing just 10% of body weight can reduce knee pain by up to 50% in overweight patients [1].
Why it matters so much for knees: Because of biomechanics. When you walk, the force across your knee is roughly 2-3 times your body weight. When you climb stairs, it’s 4-5 times. Losing 10 pounds means 30-60 pounds less force on your knee with every step.
Practical approach: Combine dietary changes with the exercise program above. Even modest weight loss (5-10%) produces clinically meaningful improvements in pain and function.
3. Oral Medications (NSAIDs and Analgesics)
The evidence: Nonsteroidal anti-inflammatory drugs (NSAIDs) like ibuprofen and naproxen remain a first-line pharmacologic treatment for knee OA. They reduce both pain and inflammation. Topical NSAIDs (diclofenac gel) are recommended as a safer alternative for patients over 65 due to lower risk of gastrointestinal and cardiovascular side effects [2].
Options include:
- Oral NSAIDs: Ibuprofen, naproxen, meloxicam — effective but carry GI and cardiovascular risks with long-term use
- Topical NSAIDs: Diclofenac gel (Voltaren) — available OTC, lower systemic side effects, recommended for older adults
- Acetaminophen (Tylenol): Provides modest pain relief but does not address inflammation; recent guidelines have moved away from strong recommendations [2]
- Duloxetine (Cymbalta): An antidepressant with FDA approval for chronic musculoskeletal pain, including knee OA
Limitations: Medications manage symptoms but do not modify disease progression. Long-term NSAID use carries real risks — GI bleeding, kidney damage, and cardiovascular events — particularly in seniors. Medications are a bridge, not a destination.
4. Bracing and Assistive Devices
The evidence: A meta-analysis of nearly 10,000 patients found that knee braces were among the most effective non-drug therapies for knee OA [4]. Unloader braces, which shift mechanical load away from the damaged compartment of the knee, can meaningfully reduce pain and delay surgery [5].
Types of braces:
- Unloader braces: Most effective for unicompartmental OA (damage primarily on one side of the knee)
- Compression sleeves: Provide proprioceptive feedback and mild support
- Patellar stabilizers: Help with kneecap tracking problems
Assistive devices: A cane used in the opposite hand reduces knee joint load by approximately 10%. Cushioned or rocker-bottom shoes can also decrease impact forces.
5. Corticosteroid Injections
The evidence: Corticosteroid (cortisone) injections provide rapid anti-inflammatory relief and are conditionally recommended for knee OA, particularly during acute flare-ups [2]. Pain reduction is typically significant within 48 hours.
Duration: This is the limitation. Effects generally last only 2-3 weeks [6], and studies show diminishing returns with repeated injections. A landmark 2-year randomized trial found that repeated corticosteroid injections were associated with greater cartilage loss compared to saline injections [7].
Best use: Cortisone is most valuable as a short-term bridge — to control a severe flare so you can participate in physical therapy, or to provide temporary relief while planning a longer-term treatment. It is not an effective long-term osteoarthritis knee treatment strategy.
For a detailed comparison of your injection options, see our cortisone vs. gel injection guide.
6. Gel Injections (Viscosupplementation)
The evidence: Viscosupplementation involves injecting hyaluronic acid (HA) — a naturally occurring component of healthy joint fluid — directly into the knee to restore lubrication and cushioning. This is the osteoarthritis treatment without surgery that bridges the gap between conservative care and joint replacement.
A real-world study tracking 782 patients across 16 clinics over six years provides the clearest efficacy picture [8]:
- 38% average pain improvement after a single treatment course
- 73.6% of patients achieved at least 50% pain reduction
- 88.7% overall satisfaction rate
- 66% pain improvement after four treatment courses (cumulative benefit)
Additional evidence: a comprehensive systematic review found that viscosupplementation is more effective than NSAIDs and corticosteroids for both pain reduction and functional improvement [9]. A separate study demonstrated that 75% of patients receiving HA injections delayed total knee replacement by 7 or more years [9].
How it works:
In a healthy knee, synovial fluid is rich in hyaluronic acid, giving it a thick, viscous quality that lubricates and cushions the joint. Osteoarthritis degrades this fluid — it becomes thinner, less effective, and reduced in volume. Viscosupplementation replenishes what the disease takes away:
- Restores lubrication for smoother joint movement
- Provides shock absorption to reduce bone-on-bone impact
- Reduces inflammation by modifying the joint’s biochemical environment
- May stimulate natural HA production by the synovial membrane [9]
- May protect remaining cartilage from further degradation
Duration of relief: Benefits typically peak between 4-12 weeks and can last 6-9 months or longer. Patients who undergo repeated treatment courses every 6 months show progressively better outcomes [8].
Who benefits most: Patients with KL Grade 2-3 (mild to moderate) OA who have not responded adequately to exercise, weight management, and medications. However, even patients with Grade 4 disease can achieve meaningful relief, particularly with multiple courses.
Insurance coverage: Medicare Part B covers viscosupplementation for qualifying patients. Most private insurers also cover the procedure. See our detailed Medicare coverage guide for specifics.
7. PRP and Regenerative Therapies
The evidence: Platelet-rich plasma (PRP) therapy uses concentrated platelets from your own blood, injected into the knee to promote healing. The evidence is mixed. Some studies show PRP outperforms HA in younger patients with early-stage OA [5], while others show no significant benefit over placebo.
Current status: PRP is not covered by Medicare or most insurance plans. Costs typically range from $500-$2,000 per injection. Clinical guidelines do not yet strongly recommend PRP due to inconsistent evidence and lack of standardized preparation protocols [2]. For a comparison of regenerative options, see our gel injections vs. PRP and stem cells page.
Bottom line: PRP may hold promise for younger patients with early disease, but it remains experimental relative to viscosupplementation, which has decades of clinical evidence and insurance coverage.
When Is Knee Surgery Necessary?
Surgery is not the enemy — it’s an important tool when the right time comes. I believe in honest conversations with patients. At Joint Relief Institute, we recommend surgical consultation when:
- Multiple courses of conservative treatment — including viscosupplementation — no longer provide adequate relief
- Pain at rest is constant and significantly impacts sleep and basic daily function
- Structural joint damage is so severe that no injection or therapy can address it
- Quality of life would clearly be better served by joint replacement
The most common surgical option is total knee arthroplasty (TKA), which replaces damaged joint surfaces with metal and plastic components. Modern knee replacements last 15-25 years, and outcomes are generally excellent when the timing is right [10].
The critical point: Trying non-surgical osteoarthritis treatment first does not mean choosing instead of surgery. It means exploring low-risk options that may provide years of relief — and if you eventually need replacement, you’ll have maintained better fitness, mobility, and muscle strength, which directly improves surgical outcomes and recovery.
For a detailed surgical comparison, see gel injections vs. knee surgery.
The Viscosupplementation Option: What the Evidence Shows
Because viscosupplementation sits at a critical decision point for many patients — between failed conservative care and surgical consideration — it deserves a closer look at the science.
Systematic Reviews and Meta-Analyses
The most rigorous form of medical evidence, systematic reviews, consistently support viscosupplementation for knee OA:
- A 2015 Cochrane-level analysis of 89 trials (12,667 participants) found that HA injections provide a clinically meaningful reduction in pain compared to placebo, with effects persisting for up to 26 weeks [11]
- The 2024 EUROVISCO consensus guidelines — the most current expert recommendations — confirmed that patients with moderate-to-severe OA benefit from viscosupplementation, particularly when other conservative treatments have failed and injections are placed accurately [12]
- High-molecular-weight HA formulations show superior effectiveness compared to older products, outperforming both non-selective NSAIDs and selective COX-2 inhibitors for pain relief [13]
Why Injection Accuracy Changes Everything
Here is a fact that most patients never hear: studies show that non-guided (“blind”) knee injections miss the joint space up to 30% of the time [14]. When the hyaluronic acid ends up in surrounding tissue instead of the joint cavity, it cannot do its job. This single factor explains much of the inconsistency in viscosupplementation outcomes across different studies and clinics.
Fluoroscopy-guided injection uses real-time X-ray imaging to visualize the needle entering the joint space. The physician can confirm accurate placement before delivering the medication. Research confirms that fluoroscopy-guided injections produce significantly better pain relief and functional outcomes compared to blind technique [14].
This is especially critical for patients with advanced OA. In a severely narrowed joint, the target space may be only a few millimeters wide. Without imaging guidance, the odds of missing increase substantially.
Multiple Gel Formulations: Not One-Size-Fits-All
There are over 12 FDA-approved hyaluronic acid products for knee OA, and they are not interchangeable. They differ in molecular weight, cross-linking, injection schedule (single vs. 3-5 weekly injections), and concentration. Having access to multiple options allows the treating physician to match the formulation to the individual patient’s disease stage, joint anatomy, and response history.
What to Expect at Joint Relief Institute
If you’re considering viscosupplementation as part of your osteoarthritis knee treatment plan, here is what a typical visit looks like:
Before Your Visit
- Insurance verification — our team confirms coverage before you come in. Medicare Part B covers viscosupplementation for qualifying patients
- Medical records review — bring X-rays or MRI reports if available. If not, we can obtain imaging
- Medication review — let us know about blood thinners or other medications that may need adjustment
During the Procedure
- Duration: Approximately 20 minutes from start to finish
- Imaging: Every injection is performed under fluoroscopy (real-time X-ray) guidance — no blind injections, ever
- Selection: We choose from 12+ FDA-approved gel formulations based on your specific condition
- Comfort: The procedure involves minimal discomfort, comparable to a routine injection
- Activity: You can walk out and resume normal activities the same day. No downtime required
After Treatment
- You may experience mild swelling or warmth at the injection site for 24-48 hours
- Benefits typically begin within 2-4 weeks and peak at 4-12 weeks
- A follow-up evaluation monitors your response and determines next steps
- Repeat treatment can be administered every 6 months if needed
Our Track Record
- 400,000+ procedures performed since 2015
- 5,800+ five-star reviews with a 4.9 Google rating across all locations
- 3 convenient Chicago-area locations: Orland Park, Oak Brook, and Glenview
- Specialization: Our physicians focus exclusively on non-surgical joint injection therapy — knees and shoulders
Frequently Asked Questions
What is the best treatment for osteoarthritis in the knees?
There is no single “best” treatment — the most effective approach depends on your disease stage, overall health, and treatment goals. Clinical guidelines recommend a stepped approach: start with exercise, weight management, and physical therapy. Add medications as needed. When conservative measures are insufficient, viscosupplementation (gel injections) provides the longest-lasting non-surgical relief, with studies showing 6-9 months of improvement per treatment course [8][9]. Surgery is reserved for cases where all conservative options have been exhausted.
Does arthritis in the knee ever go away?
No. Osteoarthritis is a progressive, degenerative condition — cartilage damage cannot be reversed with current treatments. However, progression can be significantly slowed, and symptoms can be effectively managed for years or even decades with the right combination of treatments. Many of our patients maintain active, fulfilling lives without surgery through ongoing viscosupplementation and lifestyle management.
What stage of osteoarthritis requires knee replacement?
There is no absolute stage that “requires” surgery. Many patients with KL Grade 4 (severe) OA manage well with viscosupplementation and other conservative treatments [8]. Surgery is typically recommended when pain is constant (including at rest), daily function is severely limited despite exhausting non-surgical options, and the patient’s quality of life would clearly improve with joint replacement [10]. The decision is clinical, not purely radiographic — some patients with severe X-ray findings have tolerable symptoms, while others with moderate findings are significantly disabled.
Is walking good for knee arthritis?
Yes. Walking is one of the most recommended exercises for knee osteoarthritis. Research shows that regular walking reduces pain, improves function, and may slow disease progression [4]. The key is consistency and appropriate intensity — walk on flat, even surfaces, wear supportive shoes, and start with shorter distances if you have significant pain. Walking does not “wear out” arthritic knees. In fact, the joint cartilage depends on regular movement to receive nutrients and stay healthy.
How long do gel injections last for knee osteoarthritis?
Most patients experience relief for 6-9 months per treatment course, with benefits peaking between 4-12 weeks after injection [8][9]. Duration varies based on OA severity, which gel formulation is used, and injection accuracy. Patients who undergo fluoroscopy-guided injections typically experience longer-lasting relief because the medication is verified to reach the joint space [14]. Repeated courses every 6 months produce cumulative benefits, with patients reporting progressively better outcomes over time [8].
Are osteoarthritis knee treatments covered by Medicare?
Most evidence-based osteoarthritis treatments are covered by Medicare. Physical therapy, oral medications, cortisone injections, and viscosupplementation are all covered under Medicare Part B for qualifying patients. PRP and stem cell therapies are generally not covered. At Joint Relief Institute, we verify your coverage before treatment and work to minimize out-of-pocket costs.
Take the Next Step Toward Lasting Knee Relief
If knee osteoarthritis is limiting your life, you have more options than you may realize — and surgery is rarely the only answer. The key is matching the right treatment to your specific stage of disease, with physicians who specialize in non-surgical joint care.
At Joint Relief Institute, we’ll evaluate your condition, review your imaging, verify your insurance, and give you an honest recommendation — even if that means referring you to a surgeon. We’ve helped over 40,000 patients make informed decisions about their knee pain.
Call (800) 238-9307 today to schedule your evaluation at one of our three Chicago-area locations:
- Orland Park, IL
- Oak Brook, IL
- Glenview, IL
We accept Medicare and most insurance plans.
Sources
-
Frontiers in Medicine. “Recent advances in the management of knee osteoarthritis: a narrative review.” January 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC11790583/
-
Current Orthopaedic Practice. “Current Non-surgical Management of Knee Osteoarthritis.” July 2023. https://pmc.ncbi.nlm.nih.gov/articles/PMC10370281/
-
Kellgren JH, Lawrence JS. “Radiological assessment of osteo-arthrosis.” Annals of the Rheumatic Diseases. 1957;16(4):494-502. https://pubmed.ncbi.nlm.nih.gov/13498604/
-
ScienceDaily. “Simple therapies outperform drugs for knee arthritis pain relief.” September 2025. https://www.sciencedaily.com/releases/2025/09/250919085252.htm
-
Johns Hopkins Medicine. “Knee Replacement Alternatives to Consider.” 2025. https://www.hopkinsmedicine.org/health/treatment-tests-and-therapies/knee-replacement-alternatives-to-consider
-
Current Orthopaedic Practice. “Duration and efficacy of intra-articular corticosteroid injections for knee osteoarthritis.” July 2023. https://pmc.ncbi.nlm.nih.gov/articles/PMC10370281/
-
McAlindon TE, et al. “Effect of Intra-articular Triamcinolone vs Saline on Knee Cartilage Volume and Pain in Patients With Knee Osteoarthritis: A Randomized Clinical Trial.” JAMA. 2017;317(19):1967-1975. https://pubmed.ncbi.nlm.nih.gov/28510679/
-
Long-Term Outcomes of Single versus Multiple Courses of Viscosupplementation for Osteoarthritic Knee Pain: Real-World, Multi-Practice Experience Over a Six-Year Period. PMC, 2021. https://pmc.ncbi.nlm.nih.gov/articles/PMC8364370/
-
Orthopedic Research and Reviews. “A Comprehensive Review of Viscosupplementation in Osteoarthritis of the Knee.” October 2021. https://pmc.ncbi.nlm.nih.gov/articles/PMC8567800/
-
American Academy of Orthopaedic Surgeons. “Total Knee Replacement.” OrthoInfo, 2024. https://orthoinfo.aaos.org/en/treatment/total-knee-replacement/
-
Bannuru RR, et al. “Therapeutic trajectory of hyaluronic acid versus corticosteroids in the treatment of knee osteoarthritis: a systematic review and meta-analysis.” Arthritis & Rheumatism. 2009;61(12):1704-1711. https://pubmed.ncbi.nlm.nih.gov/19950318/
-
EUROVISCO Consensus Guidelines for the Use of Hyaluronic Acid Viscosupplementation in Knee Osteoarthritis Based on Patient Characteristics. Journal of Orthopaedic Surgery and Research, 2024. https://journals.sagepub.com/doi/10.1177/19476035241271970
-
Concoff A, et al. “Efficacy and safety of high-molecular-weight hyaluronic acid for knee osteoarthritis.” Osteoarthritis and Cartilage. 2017;25(Suppl 1):S165-S166.
-
National Center for Biotechnology Information. “Fluoroscopic-guided procedures of the lower extremity.” August 2022. https://pmc.ncbi.nlm.nih.gov/articles/PMC9362560/


